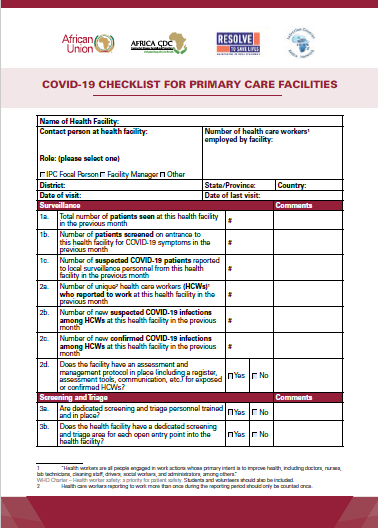
Name of Health Facility:
Contact person at health facility: Number of health care workers employed by facility:
Role: (please select one)
X- IPC Focal Person X- Facility Manager X- Other
District: State/Province: Country:
Date of visit: Date of last visit:
Surveillance
1a. Total number of patients seen at this health facility in the previous month #
1b. Number of patients screened on entrance to this health facility for COVID-19 symptoms in the previous month
1c. Number of suspected COVID-19 patients reported to local surveillance personnel from this health facility in the previous month
2a. Number of unique2 health care workers (HCWs) who reported to work at this health facility in the previous month
2b. Number of new suspected COVID-19 infections among HCWs at this health facility in the previous month
2c. Number of new confirmed COVID-19 infections among HCWs at this health facility in the previous month
2d. Does the facility have an assessment and management protocol in place (including a register, assessment tools, communication, etc.) for exposed or confirmed HCWs?
| File | Action |
|---|
| COVID-19 CHECKLIST FOR PRIMARY CARE FACILITIES – May24 | Download |